

Last Updated: March 2026 | v1.0
BPC-157 and TB-500 are the two most frequently studied peptides in preclinical tissue repair research. Both compounds appear in published studies examining wound healing, tendon recovery, and inflammatory modulation — but they operate through fundamentally different biological mechanisms. BPC-157 (Body Protection Compound-157) is a 15-amino-acid synthetic peptide derived from human gastric juice that primarily promotes angiogenesis through VEGF upregulation. TB-500 is a synthetic 43-amino-acid fragment of thymosin beta-4, a naturally occurring protein that regulates actin polymerization and cell migration. Understanding how these mechanisms differ — and where they overlap — helps researchers design more informed protocols. This guide compares the two compounds across mechanism, published literature, reconstitution, and research dosage parameters. All products and information are provided for laboratory and research purposes only.
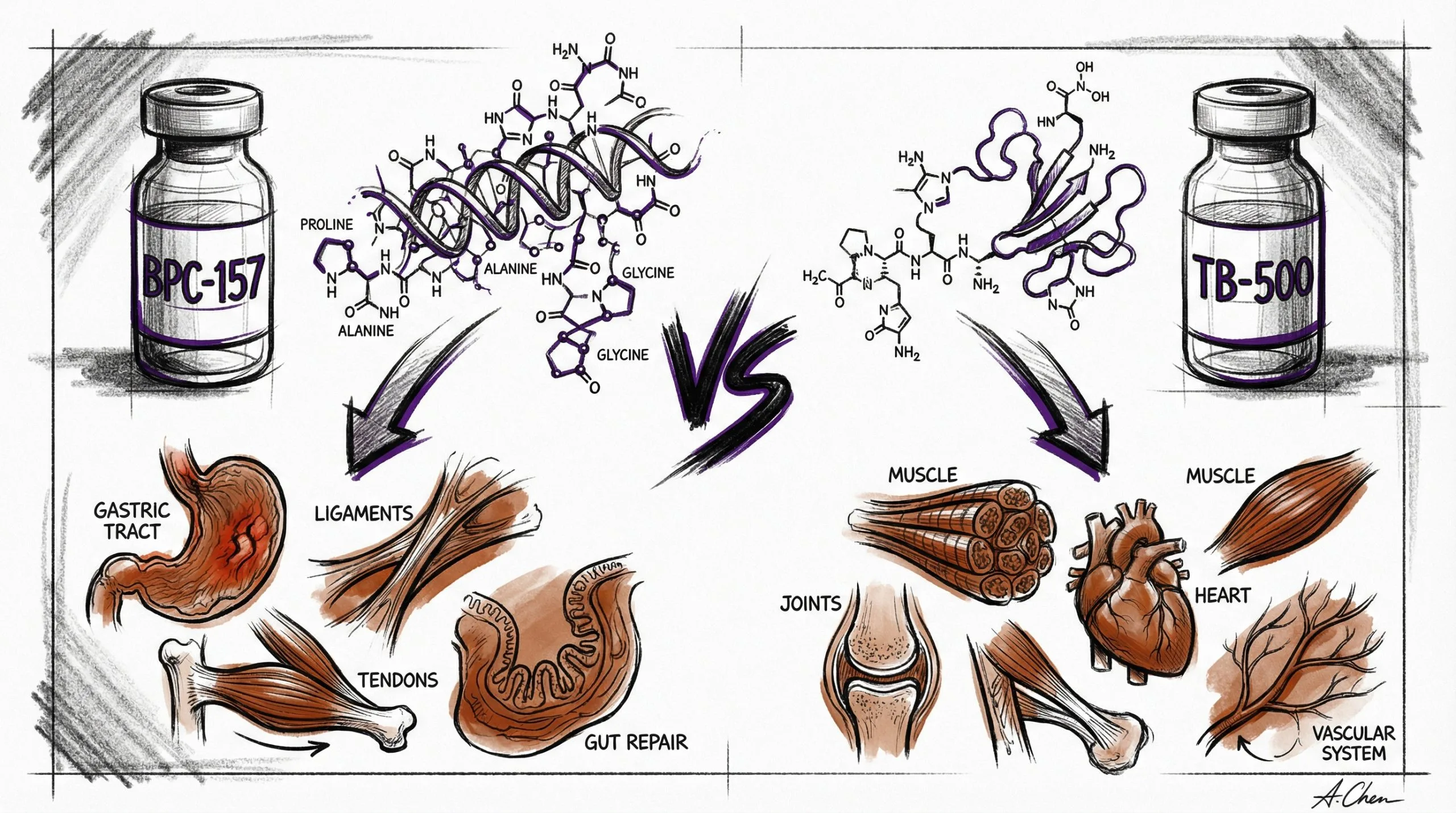
Quick Comparison: BPC-157 vs TB-500
- BPC-157: 15 amino acids, 1,419 Da, promotes angiogenesis via VEGF, gastric acid stable
- TB-500: 43 amino acids, 4,963 Da, regulates actin/cell migration via thymosin beta-4 pathway
- Overlap: Both studied in tendon, muscle, and wound healing models with positive preclinical outcomes
- Key difference: BPC-157 builds new blood vessels to injury sites; TB-500 mobilizes cells to migrate into damaged tissue
- Combined use: Some published protocols study both compounds together for complementary pathway coverage
Use the free reconstitution calculator for exact syringe units, or browse the peptide reference library for dosing and protocol data.
How Do the Mechanisms of Action Differ?
BPC-157’s primary mechanism centers on vascular endothelial growth factor (VEGF) upregulation. Published studies suggest that BPC-157 increases VEGFR2 expression in endothelial cells, stimulating the formation of new blood vessels (angiogenesis) at injury sites (PubMed: 24186207). This increased vascularization delivers oxygen, nutrients, and immune cells to damaged tissue — the foundational requirement for repair. BPC-157 also modulates the nitric oxide (NO) system, influencing vasodilation and inflammatory signaling. For a complete mechanism breakdown, see our BPC-157 Research Guide.
TB-500 operates through a different pathway entirely. As a synthetic fragment of thymosin beta-4 (Tβ4), TB-500 regulates actin polymerization — the assembly of actin filaments that form the structural skeleton of cells. By sequestering G-actin monomers, TB-500 promotes actin cytoskeleton remodeling, which enables cell migration, differentiation, and proliferation at wound sites (PubMed: 20614940). In practical terms, BPC-157 builds the vascular infrastructure to support healing, while TB-500 mobilizes the cellular workforce that performs the repair. This mechanistic distinction is why some researchers study both compounds in combination protocols.
What Does the Published Research Show for Each Compound?
BPC-157 has a larger body of published preclinical literature, with over 100 studies indexed on PubMed. The strongest evidence clusters around tendon repair (Achilles tendon transection models showing accelerated functional recovery), gastrointestinal protection (gastric ulcer models demonstrating accelerated mucosal healing), and musculoskeletal injury (crushed muscle models with enhanced satellite cell activation). BPC-157’s gastric acid stability is a unique property — it retains biological activity at pH 2-3, enabling both systemic and oral administration routes in published protocols (PubMed: 25415894).
TB-500’s published literature is smaller but well-characterized, with key studies focusing on dermal wound healing, cardiac tissue repair, and corneal healing models. A landmark study demonstrated that thymosin beta-4 promoted cardiomyocyte migration and survival in murine cardiac injury models (PubMed: 15340520). In dermal wound models, TB-500 accelerated wound closure rates through enhanced keratinocyte migration (PubMed: 17318735). TB-500 has also been studied in hair follicle stem cell models, where it promoted hair growth through beta-4-mediated cell migration signaling.
How Do Reconstitution Protocols Compare?
Both peptides follow standard reconstitution procedures using bacteriostatic water (BAC water), but their typical vial sizes and resulting concentrations differ slightly.
BPC-157 reconstitution: A standard 10 mg vial reconstituted with 2 mL of BAC water yields a concentration of 5,000 mcg/mL. At this concentration, each unit on a 100-unit insulin syringe equals 50 mcg. For a research dosage of 500 mcg, researchers draw 10 units. The reconstituted solution is stored at 2-8 °C (36-46 °F) and remains stable for approximately 21-28 days.
TB-500 reconstitution: A standard 10 mg vial reconstituted with 2 mL of BAC water yields the same concentration of 5,000 mcg/mL. The per-unit calculation is identical: each syringe unit equals 50 mcg. For a research dosage of 500 mcg, researchers draw 10 units. Storage conditions are the same as BPC-157: 2-8 °C (36-46 °F) for up to 28 days post-reconstitution.
Both compounds should be reconstituted by injecting BAC water slowly along the vial wall, allowing 2-3 minutes for dissolution, and gently rolling — never shaking — to mix. For step-by-step instructions, see our Peptide Reconstitution 101 guide, or use the reconstitution calculator at HowToMixPeptides.com.
How Do Research Dosages and Protocols Compare?
| Parameter | BPC-157 | TB-500 |
|---|---|---|
| Vial size | 10 mg | 10 mg |
| BAC water volume | 2 mL | 2 mL |
| Research dosage | 500 mcg | 500 mcg |
| Syringe units | 10 units | 10 units |
| Timing | AM/PM (twice daily) | AM (once daily) |
| Frequency | Daily | Daily |
| Cycle | 8 weeks on / 8 weeks off | 8 weeks on / 8 weeks off |
The primary protocol difference is administration frequency: BPC-157 is commonly referenced at twice daily (AM/PM) while TB-500 is typically referenced at once daily (AM). This distinction appears in multiple published protocols, though the optimal frequency for either compound has not been established through controlled clinical trials.
Can BPC-157 and TB-500 Be Used Together in Research?
Yes — combined protocols are documented in the published literature and represent a common approach in preclinical research. The rationale is mechanistic complementarity: BPC-157’s angiogenic effects (building vascular infrastructure) and TB-500’s cell migration effects (mobilizing repair cells) address different stages of the tissue repair cascade. Peptideware also carries a pre-blended BPC-157/TB-500 formulation for researchers who prefer standardized combination dosing.
When studied separately but concurrently, researchers typically administer each compound at its standard research dosage. Published combination protocols generally describe BPC-157 at 250-500 mcg and TB-500 at 250-500 mcg, administered at the same or different injection sites. The blend calculator at HowToMixPeptides.com provides concentration and unit calculations for combined protocols.
Which Compound Is More Studied for Specific Research Areas?
Tendon and ligament repair: BPC-157 has more published data in this area, with multiple studies on Achilles tendon, MCL, and patellar tendon models. TB-500 has been studied in tendon contexts but with fewer dedicated publications.
Cardiac tissue research: TB-500 (via thymosin beta-4) has stronger published evidence for cardiac applications, including cardiomyocyte survival and migration studies. BPC-157 has limited published data in cardiac models.
Gastrointestinal research: BPC-157 dominates this category with extensive gastric ulcer, colitis, and anastomosis studies. TB-500 has minimal published GI research.
Wound healing (dermal): Both compounds show positive preclinical results. TB-500’s keratinocyte migration data is particularly well-characterized. BPC-157’s angiogenic mechanism also supports dermal repair through increased blood supply.
Neuroprotection: BPC-157 has more published data on dopaminergic and serotonergic modulation. TB-500 has emerging neuroprotective research but a smaller evidence base in this area.
Frequently Asked Questions
What is the main difference between BPC-157 and TB-500?
BPC-157 primarily promotes angiogenesis (new blood vessel formation) through VEGF upregulation, while TB-500 regulates actin polymerization to promote cell migration and tissue remodeling. They target different stages of the tissue repair process.
Can both peptides be reconstituted with the same bacteriostatic water?
Yes. Both BPC-157 and TB-500 are reconstituted using bacteriostatic water with 0.9% benzyl alcohol. The same BAC water vial can be used for both peptides — use a fresh, sterile syringe for each vial to prevent cross-contamination.
Which peptide has more published research?
BPC-157 has a significantly larger body of published literature, with over 100 preclinical studies on PubMed. TB-500 (thymosin beta-4) has a substantial but smaller body of published work, with strongest evidence in cardiac and dermal wound models.
Do researchers ever combine BPC-157 and TB-500?
Yes. Combined protocols are documented in published literature. The rationale is mechanistic complementarity — BPC-157 builds vascular infrastructure while TB-500 mobilizes repair cells. Both compounds can be administered concurrently at their standard research dosages.
Is one peptide more stable than the other?
BPC-157 has a notable advantage in gastric acid stability, retaining activity at pH 2-3. TB-500 does not share this property. Both peptides have similar stability once reconstituted: 21-28 days at 2-8 °C (36-46 °F) in bacteriostatic water.
Where can I find both peptides with third-party testing?
Peptideware provides both BPC-157 (10 mg) and TB-500 (10 mg) with independent HPLC and mass spectrometry verification. COAs are published on each product page.
For research purposes only. All products and information are provided for laboratory and research purposes only.
