

Last Updated: May 15, 2026 | v1.0
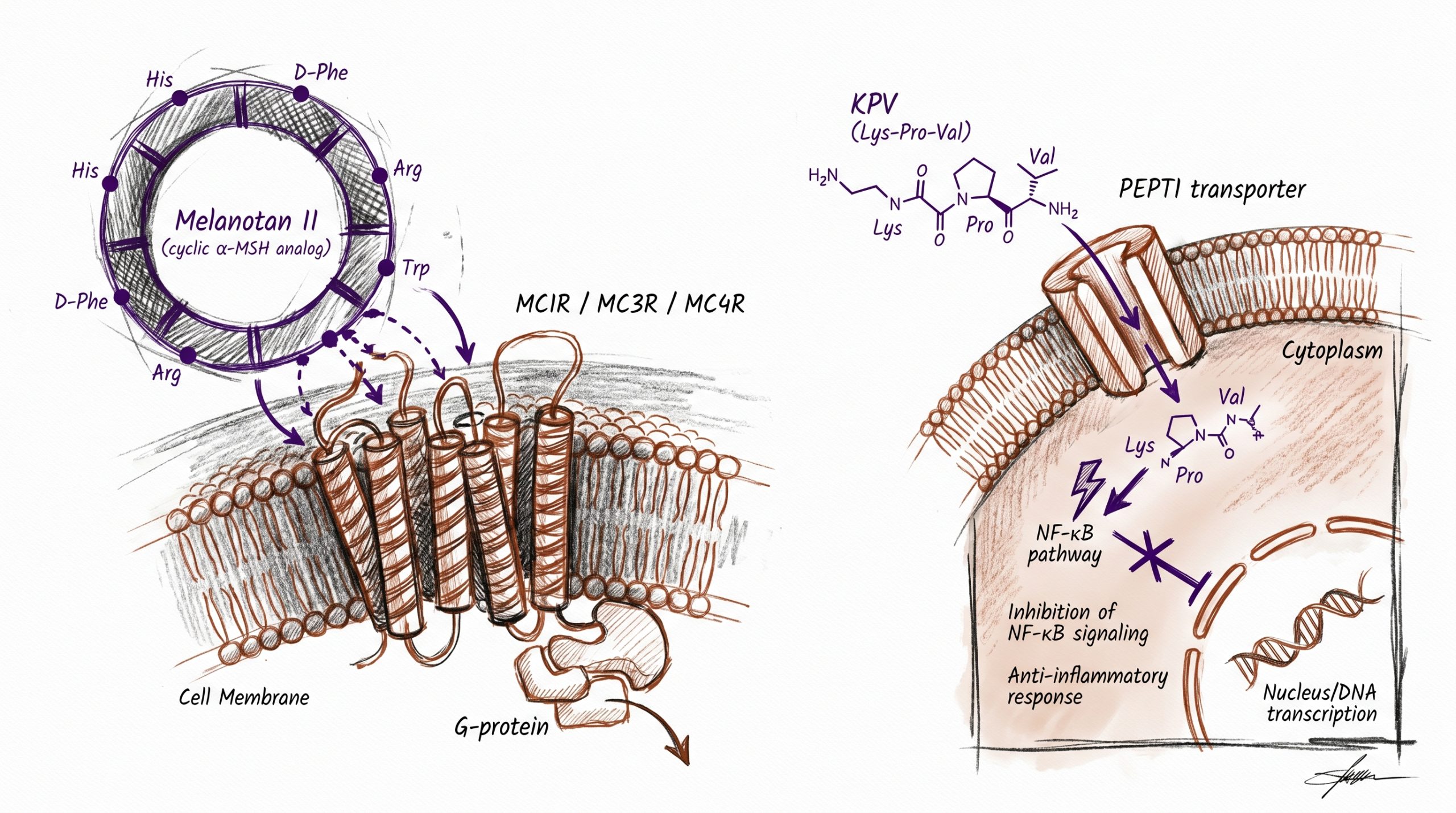
Melanotan II and KPV are two research peptides that both derive their structural lineage from alpha-melanocyte stimulating hormone (α-MSH), but they engage cellular biology through fundamentally opposite mechanisms. Melanotan II is a cyclic synthetic heptapeptide analog of α-MSH designed for receptor-level potency, and it binds the melanocortin receptor family (MC1R through MC5R) as a non-selective agonist. KPV is the linear C-terminal tripeptide of α-MSH (residues 11–13: lysine-proline-valine), and its anti-inflammatory activity in published research is melanocortin-receptor-independent, acting on intracellular inflammatory signaling rather than the MC receptors themselves. One molecule is a cell-surface receptor agonist; the other is a small bioactive fragment whose anti-inflammatory action bypasses receptor pharmacology entirely. This guide compares the two compounds for researchers selecting between melanocortin-system receptor pharmacology and α-MSH-derived anti-inflammatory tripeptide research. All products and information are provided for laboratory and research purposes only.
Quick Comparison: Melanotan II vs KPV
| Attribute | Melanotan II | KPV |
|---|---|---|
| Chemical class | Cyclic synthetic heptapeptide α-MSH analog | Linear α-MSH C-terminal tripeptide fragment |
| Sequence | Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-NH2 | Lys-Pro-Val (residues 11–13 of α-MSH) |
| Molecular weight | ~1,024 Da | ~343 Da |
| Origin | Designed at the University of Arizona (Hadley laboratory), late 1980s | α-MSH fragment chemistry characterized from the 1990s onward in inflammation research |
| Primary molecular target | Melanocortin receptors MC1R, MC3R, MC4R, MC5R (non-selective agonist) | Intracellular inflammatory signaling (NF-κB pathway in published cellular models); melanocortin-receptor-independent |
| Reported preclinical effects | Stimulated melanogenesis (MC1R), appetite reduction (MC4R), erectile response in rodent and early human studies (MC4R) | Reduced inflammatory readouts in DSS-colitis mouse models and cellular inflammation assays; mast-cell stabilization in published reports |
| Route in published research | Subcutaneous in published rodent and early-phase human studies | Oral (PEPT1 uptake), intraperitoneal, and topical in published model systems |
| Receptor pharmacology | Cell-surface GPCR agonism; cAMP signaling downstream of MC receptors | Intracellular; PEPT1-mediated uptake then cytoplasmic action |
| Literature focus | Pigmentation biology, MC receptor pharmacology, appetite and sexual-response models | Inflammatory bowel disease, mucosal inflammation, atopic and allergic models |
What Is Melanotan II and How Does It Engage the Melanocortin System?
Melanotan II is a cyclic heptapeptide synthetic analog of alpha-melanocyte stimulating hormone (α-MSH) designed at the University of Arizona in the late 1980s by the Hadley research group as a tool to probe melanocortin receptor pharmacology. The native α-MSH sequence (Ser-Tyr-Ser-Met-Glu-His-Phe-Arg-Trp-Gly-Lys-Pro-Val) is rapidly degraded in plasma and has only modest receptor potency in many in vivo settings, which limited its utility as a research tool. Melanotan II addressed both constraints through two structural modifications: introduction of a non-natural amino acid (norleucine substitution for methionine at position 4) and cyclization through a lactam bridge between the side chains at positions 5 and 10 (Ac-Nle-c[Asp-His-D-Phe-Arg-Trp-Lys]-NH2). The result is a peptide with markedly increased metabolic stability and receptor affinity relative to native α-MSH, and it became a standard research tool for melanocortin biology. Researchers studying MC receptor pharmacology can source Melanotan II from Peptideware as a 10 mg lyophilized preparation with batch-specific analytical documentation.
Melanotan II is a non-selective melanocortin receptor agonist, meaning it binds and activates four of the five melanocortin receptor subtypes — MC1R, MC3R, MC4R, and MC5R — with comparable affinity. Each receptor maps to a distinct preclinical research domain. MC1R is expressed on epidermal melanocytes and drives melanogenesis (eumelanin synthesis) when activated; the published reports of pigmentation responses to Melanotan II in rodent and early human studies derive from this MC1R agonism. MC3R and MC4R are central-nervous-system receptors involved in energy balance and feeding behavior; MC4R agonism has been associated with reduced food intake in rodent appetite studies and with erectile response in published rodent and early-phase human research. MC5R is expressed in exocrine tissues and has been associated with sebum secretion in some models. The companion Melanotan II Research Guide covers melanocortin system pharmacology, published receptor binding data, and protocol considerations in greater depth.
What Is KPV and Why Is Its Activity Melanocortin-Receptor-Independent?
KPV is the linear tripeptide consisting of lysine, proline, and valine (Lys-Pro-Val) — the three C-terminal amino acid residues of α-MSH (positions 11–13). Although KPV is a structural fragment of α-MSH, its activity in published anti-inflammatory research does not depend on the melanocortin receptor family. This was demonstrated in studies that retained KPV’s anti-inflammatory effect in cellular and animal models lacking functional melanocortin receptors or treated with MC receptor antagonists, and in studies showing KPV uptake through the peptide transporter PEPT1 rather than through MC receptor binding at the cell surface. The functional implication is that KPV represents a mechanistically distinct compound from receptor-targeted melanocortin agonists like Melanotan II, despite sharing the α-MSH structural lineage. Researchers studying α-MSH–derived tripeptide anti-inflammatory biology can source KPV from Peptideware, supplied as a 10 mg lyophilized preparation with analytical documentation. The dedicated KPV Research Guide details fragment chemistry, published anti-inflammatory models, and protocol considerations.
The mechanistic literature on KPV is anchored in inflammatory bowel disease (IBD) research. Published preclinical work has shown that orally administered KPV reduces inflammatory readouts — pro-inflammatory cytokine production, leukocyte infiltration, and histopathological damage scores — in dextran sulfate sodium (DSS) and trinitrobenzene sulfonic acid (TNBS) mouse models of colitis. The proposed mechanism in published reports involves intracellular suppression of NF-κB pathway activation in immune cells, with reductions in downstream inflammatory cytokines including TNF-α, IL-6, and IL-1β. Importantly for protocol design, KPV uptake through PEPT1 — the brush-border peptide transporter expressed in intestinal epithelium and elsewhere — supports oral-route administration with intracellular delivery, which is unusual for a peptide at this molecular weight and contributes to its preclinical research interest in mucosal-inflammation models. Mast-cell stabilization and reduced histamine release have also been reported in published in vitro work, extending the anti-inflammatory profile to allergic and atopic models.
How Do Their Mechanisms Diverge Beyond the Shared α-MSH Lineage?
The most important conceptual distinction between Melanotan II and KPV is the cellular layer at which each compound operates. Melanotan II is a receptor agonist: it binds melanocortin receptors at the cell surface, stabilizes their active conformation, and activates G-protein-coupled downstream signaling (primarily through Gαs-mediated cyclic AMP production at MC1R, MC3R, MC4R, and MC5R). The biological output depends on which cells express which receptor subtypes — melanocytes express MC1R, central neurons express MC4R, and so on — and on the magnitude of cAMP signaling triggered by receptor activation. KPV is an intracellular agent: it enters cells through PEPT1-mediated uptake and acts on cytoplasmic and nuclear inflammatory signaling proteins, with NF-κB suppression as the most-cited mechanism in published reports. The downstream biology of KPV does not require any cell-surface receptor binding, and KPV has no characterized agonist activity at any of the melanocortin receptors that Melanotan II targets.
This mechanistic divergence translates directly into the design of research protocols. Investigators using Melanotan II construct receptor-pharmacology experiments — receptor binding affinity studies, cAMP accumulation assays, agonist–antagonist competition with MC receptor blockers like SHU9119 or HS024, and in vivo phenotype studies that map receptor-specific responses (pigmentation for MC1R, appetite for MC4R). Investigators using KPV construct inflammation-pharmacology experiments — colitis induction models, NF-κB reporter assays, mast cell degranulation experiments, and pro-inflammatory cytokine quantification in tissue homogenates. The two literatures rarely overlap. A researcher studying melanocortin receptor agonism would not substitute KPV for Melanotan II; a researcher studying tripeptide anti-inflammatory biology would not substitute Melanotan II for KPV. The shared α-MSH lineage is structural, not pharmacological. The pillar overview Healing Peptides: BPC-157, TB-500, GHK-Cu, and Regenerative Research places KPV in the broader anti-inflammatory and mucosal-healing context.
| Compound | Mode of action | Representative preclinical findings | Primary research literature |
|---|---|---|---|
| Melanotan II | Non-selective melanocortin receptor agonist (MC1R/MC3R/MC4R/MC5R); cAMP signaling at the cell surface | Stimulated melanogenesis in rodent and early human studies (MC1R); appetite reduction and erectile response in rodent models (MC4R) | Pigmentation biology, MC receptor pharmacology, central-nervous-system feeding and sexual-response models |
| KPV | Intracellular anti-inflammatory action after PEPT1-mediated uptake; NF-κB pathway suppression in published cellular models; melanocortin-receptor-independent | Reduced inflammatory readouts in DSS and TNBS colitis mouse models; mast-cell stabilization and reduced histamine release in vitro | Inflammatory bowel disease, mucosal-inflammation models, allergic and atopic inflammation research |
Which Compound Should Researchers Choose?
Selection between Melanotan II and KPV depends on the research question and the cellular layer under investigation. For investigators studying melanocortin receptor pharmacology, pigmentation biology, MC1R-driven melanogenesis, MC4R-related appetite or sexual-response phenotypes, or non-selective MC receptor agonism as a pharmacological probe, Melanotan II is the appropriate choice. The 10 mg preparation supports cellular receptor-binding assays, cAMP accumulation experiments, and in vivo studies in rodent models where receptor agonism is the experimental input. Investigators studying MC4R-selective pharmacology should also be aware of Bremelanotide (PT-141), a Melanotan II–derived analog with shifted selectivity that is studied for sexual-response endpoints; PT-141 is a separate research compound and is not equivalent to Melanotan II for general MC receptor pharmacology research. The related comparison GLOW vs KLOW Blend covers KPV in the context of the KLOW protocol stack (BPC-157 + TB-500 + GHK-Cu + KPV), useful for researchers evaluating combined-compound regenerative protocols.
For investigators studying anti-inflammatory tripeptide biology, NF-κB pathway suppression by α-MSH fragments, mucosal inflammation in colitis models, mast-cell stabilization, or PEPT1-mediated oral-route peptide research, KPV is the appropriate choice. The 10 mg preparation supports oral-administration protocols in rodent IBD models, cellular NF-κB reporter assays, mast cell degranulation experiments, and topical or intraperitoneal preclinical research where the tripeptide’s small size and PEPT1 substrate behavior are experimentally relevant. The companion comparison TB-500 vs BPC-157 vs KPV contrasts KPV against two systemic-healing peptides operating through distinct mechanisms (TB-500 actin sequestration; BPC-157 growth-factor and angiogenic signaling), providing a third reference point for compound selection within regenerative and anti-inflammatory research.
How Are These Compounds Reconstituted and Stored?
Melanotan II is supplied as a lyophilized peptide in sealed vials and should be stored at –20 degrees Celsius (or lower) for long-term stability, with light and moisture protection. For research use, reconstitution typically uses bacteriostatic water (0.9% benzyl alcohol) for short-term reconstituted storage at 2–8 degrees Celsius, or sterile water for single-use preparations; the cyclic structure of Melanotan II provides better aqueous stability than linear peptides at the same molecular weight, but reconstituted solutions should still be used within standard peptide-research timelines. Investigators should consult published preclinical protocols for vehicle composition and concentration specific to the assay endpoint. Peptideware supplies bacteriostatic water in 3 mL and 10 mL formats for laboratory reconstitution work.
KPV is supplied as a lyophilized peptide and should also be stored at –20 degrees Celsius for long-term stability. Reconstitution depends on the intended route in the preclinical model. For oral-administration protocols, KPV is typically dissolved in drinking water or buffered vehicle for delivery to rodents in DSS or TNBS colitis models — the small molecular size and PEPT1-mediated uptake support oral-route bioavailability that is unusual for peptides generally. For intraperitoneal or topical preclinical research, sterile water or buffered saline is the most common vehicle in published protocols. Investigators should consult the primary IBD and mucosal-inflammation literature for vehicle composition and dosing parameters specific to the target model. As with all peptide research preparations, reconstituted KPV stocks should be aliquoted to minimize freeze-thaw cycles and stored at –20 or –80 degrees Celsius for short-term re-use. The Peptide Reconstitution 101 guide covers general aqueous-reconstitution methodology applicable to both compounds.
Frequently Asked Questions
Is KPV the same as α-MSH or a melanocortin agonist?
No. KPV is the C-terminal tripeptide fragment of α-MSH (residues 11–13: lysine-proline-valine), but its anti-inflammatory activity in published research is melanocortin-receptor-independent. Studies have demonstrated KPV’s anti-inflammatory effects in cellular and animal models lacking functional melanocortin receptors or treated with MC receptor antagonists, and have characterized PEPT1-mediated intracellular uptake rather than cell-surface MC receptor binding. KPV shares α-MSH’s structural lineage but not its receptor pharmacology — it is a mechanistically distinct compound from full α-MSH or from receptor-targeted melanocortin agonists like Melanotan II.
Is Melanotan II the same as PT-141 (Bremelanotide)?
No, but they are structurally related. Bremelanotide (PT-141) is a Melanotan II–derived analog created by opening the cyclic structure of Melanotan II and modifying the C-terminus, resulting in a peptide with shifted melanocortin receptor selectivity favoring MC4R relative to MC1R. The pharmacological consequence is that PT-141 produces relatively more central-nervous-system MC4R-related effects (the basis of its sexual-response research literature) and relatively less MC1R-driven pigmentation effect than Melanotan II. Researchers should select Melanotan II for non-selective MC receptor agonism and pigmentation-biology research, and PT-141 specifically for MC4R-selective research questions. Peptideware does not currently carry PT-141; researchers requiring it should source it separately.
Can Melanotan II and KPV be combined in research protocols?
Combination research using Melanotan II and KPV has not been characterized in published preclinical literature, and no head-to-head or combination data are available. The two compounds operate on entirely different cellular layers — cell-surface melanocortin receptor agonism for Melanotan II, intracellular NF-κB pathway suppression for KPV — so a combination would test whether parallel modulation of receptor-driven cAMP signaling and intracellular inflammatory signaling produces additive or independent effects. Investigators interested in combination research should design parallel-arm studies that compare each compound alone against the combination, control for the route-of-administration difference (Melanotan II subcutaneous, KPV oral or intraperitoneal in published protocols), and consult published pharmacokinetic data for each compound before designing combination dosing protocols.
Why is KPV orally bioavailable but most peptides are not?
KPV’s oral bioavailability in published preclinical models is supported by its very small size (a tripeptide of ~343 Da) and by uptake through PEPT1, the brush-border peptide transporter that handles di- and tripeptides at the intestinal epithelium and other tissues. Most peptides at higher molecular weights — Melanotan II at ~1,024 Da, BPC-157 at ~1,419 Da, larger peptides at several kilodaltons — are not PEPT1 substrates and are degraded by intestinal proteases before they can be absorbed intact. Published oral-administration protocols for KPV in DSS and TNBS colitis mouse models exploit the PEPT1-mediated uptake mechanism to deliver intact tripeptide to the intestinal mucosa, the tissue most relevant to the IBD research literature. Researchers planning oral-route research should be aware that this property is specific to KPV (and to a small number of other di- and tripeptides) and does not generalize to most peptide research compounds.
What side effects have been reported for Melanotan II in research?
Published preclinical and early-phase human research has reported side effects associated with Melanotan II administration that include nausea (the most commonly reported, attributed to central MC4R agonism), flushing, transient blood pressure changes, and increased nevus pigmentation. Unregulated non-research use of Melanotan II has also been associated in case reports with darkening or enlargement of existing nevi, raising concerns that have been discussed in dermatological case-report literature; these reports do not establish causality but are part of the published safety context. Within research-only contexts, investigators should treat Melanotan II as a research compound, follow institutional biosafety and animal-research protocols, and consult the published pharmacology literature when designing studies. Melanotan II is not approved as a therapeutic agent in any major regulatory jurisdiction.
What purity and verification should researchers require?
Research-grade Melanotan II and KPV should be sourced from suppliers providing third-party certificate of analysis documentation. For Melanotan II, identity should be verified by HPLC purity (typically greater than 98%) and mass spectrometry confirmation at approximately 1,024 Daltons, with correct cyclic structure confirmed by retention time and fragmentation pattern. For KPV, the small molecular size makes mass-spectrometry confirmation at approximately 343 Daltons the primary identity check, alongside HPLC purity (typically greater than 98%). Both compounds should be free of detectable endotoxin contamination for in vivo preclinical use, and both should ship with batch-specific analytical documentation. The Peptideware Peptide Quality: Third-Party Testing guide describes purity standards and COA interpretation in detail.
Are these compounds approved for human use?
No. Melanotan II and KPV supplied for research are intended exclusively for laboratory and preclinical model-system use. Melanotan II is not approved as a therapeutic agent in any major regulatory jurisdiction, and the Bremelanotide (PT-141) derivative has separate regulatory status as an approved drug product for a specific clinical indication in some jurisdictions — but PT-141 is a distinct molecule and that approval does not extend to Melanotan II. KPV is a research compound that has been investigated in published preclinical inflammation research but has not undergone the regulatory process required to support clinical use. Peptideware’s products are sold with explicit research-use-only documentation, and researchers should ensure that all preclinical protocols comply with applicable institutional and regulatory requirements.
Summary
Melanotan II and KPV both trace their structural lineage to alpha-melanocyte stimulating hormone (α-MSH) but operate through fundamentally different mechanisms. Melanotan II is a cyclic synthetic heptapeptide designed at the University of Arizona in the late 1980s as a non-selective melanocortin receptor agonist; it binds MC1R, MC3R, MC4R, and MC5R, and the published research literature spans pigmentation biology, central-nervous-system appetite and sexual-response models, and MC receptor pharmacology generally. KPV is the linear tripeptide formed by the C-terminal three residues of α-MSH, and its anti-inflammatory activity in published preclinical research is melanocortin-receptor-independent, acting through intracellular NF-κB pathway suppression after PEPT1-mediated cellular uptake; the literature is anchored in inflammatory bowel disease, mucosal inflammation, and mast-cell-mediated allergic models. The two compounds occupy mechanistically non-overlapping research domains: a receptor-pharmacology probe in one case, an intracellular anti-inflammatory tripeptide in the other. Researchers selecting between them should match the compound’s mechanistic role to the research question, consult the primary literature for protocol parameters, and follow third-party COA verification standards. Both compounds are research tools only and have not been approved for human therapeutic use.
Research Disclaimer: All products are intended for laboratory and research purposes only. Not for human or animal consumption. These statements have not been evaluated by the FDA.





